
- General Dermatology
- Eczema
- Alopecia
- Aesthetics
- Vitiligo
- COVID-19
- Actinic Keratosis
- Precision Medicine and Biologics
- Rare Disease
- Wound Care
- Rosacea
- Psoriasis
- Psoriatic Arthritis
- Atopic Dermatitis
- Melasma
- NP and PA
- Skin Cancer
- Hidradenitis Suppurativa
- Drug Watch
- Pigmentary Disorders
- Acne
- Pediatric Dermatology
- Practice Management
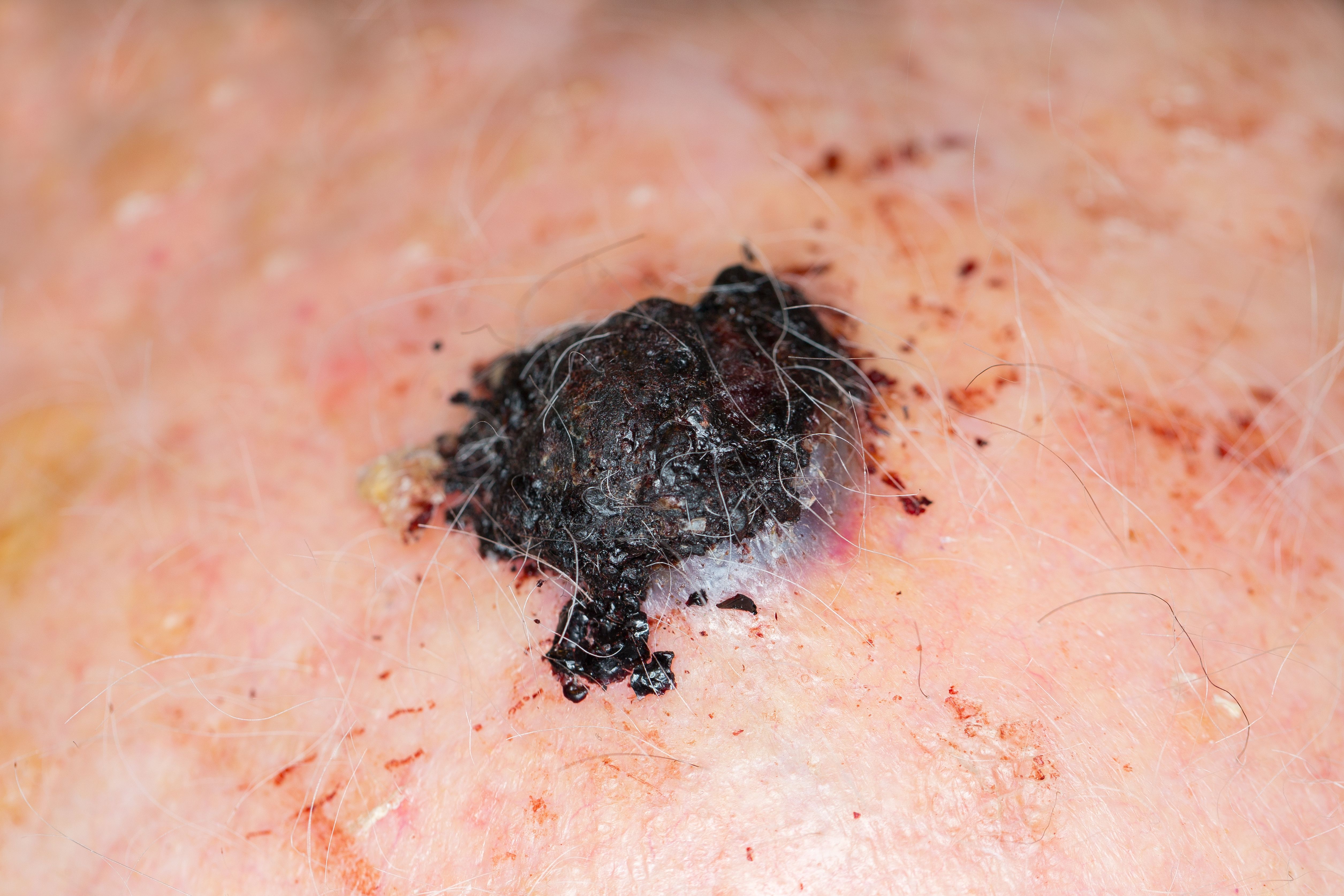
Interventions in Minimal Residual Disease Lead to Long-Term Melanoma Control
In a recent review, authors explored the effects of targeted therapies and immune checkpoint inhibitors on melanoma, particularly in minimal residual disease.
Cutaneous melanoma responds to targeted therapies (TT) and immune checkpoint inhibitors (ICI) in 3 phases, according to a recent review.1


lavizzara/AdobeStock
In the review, authors also found that TT and ICI can affect both melanoma cells and the tumor immune microenvironment, particularly in the middle of the 3 phases. These phases are known as early response, minimal residual disease (MRD), and disease progression. More specifically, the review assessed the role of TT and ICI in the MRD phase.
Historically, the developments and implementations of TT and ICI have improved patient outcomes in metastatic melanoma. However, review authors said some questions of TT and ICI sequencing remain unresolved, stating that the goal of their review was to uncover more of the biology of the 3 phases, as well as determine a correlation and response between TT, ICI, and MRD.
The MRD phase is drug-tolerant and enabled by genetic and non-genetic changes. During the process of MRD, changes may lead to TT resistance, and ultimately, to melanoma relapse.
“Based on the frequency of patients who progress after partial or complete response to ICI, we propose that a portion of patients who initially respond to ICI go on to establish MRD. These cells persist under therapeutic pressure eventually driving disease progression and secondary resistance,” authors wrote. “Following MRD or partial response, some patients acquire resistance to ICI, with 12%–38% of those who initially respond eventually progressing on therapy. Several mechanisms of acquired resistance have been identified that ultimately drive disease progression."
Additionally, authors found that during the review, cutaneous melanoma may be at its most vulnerable during the MRD process; this is due to a low tumor load. Additional therapeutic interventions may be required on a long-term basis in order for patients to avoid progression, or ultimately to lead to a clinical cure. These additional therapies can reduce the risk of melanoma relapse and recurrence under TT and ICI treatments.
“Both TT and ICI have an MRD phase from which disease relapse emerges through a host of genetic and non-genetic alterations. We suggest that further studies are needed to adequately characterize the origin and evolution of resistance during the MRD phase, for example the emergence of NCSCs, with the view to developing potentially curative treatment options,” review authors wrote. “The clonal evolution of melanoma following therapeutic intervention could be assessed through single cell-RNA sequencing or clonal mapping of serial tumour biopsies.”
Reference
- Patel RP, Somasundram PM, Smith LK, Sheppard KE, McArthur GA. The therapeutic potential of targeting minimal residual disease in melanoma. Clinical and Translational Medicine. 2023;13(3). doi:10.1002/ctm2.1197














